ehlers danlos vs marfans
- Keywords: Step 3, Allergy and Immunology
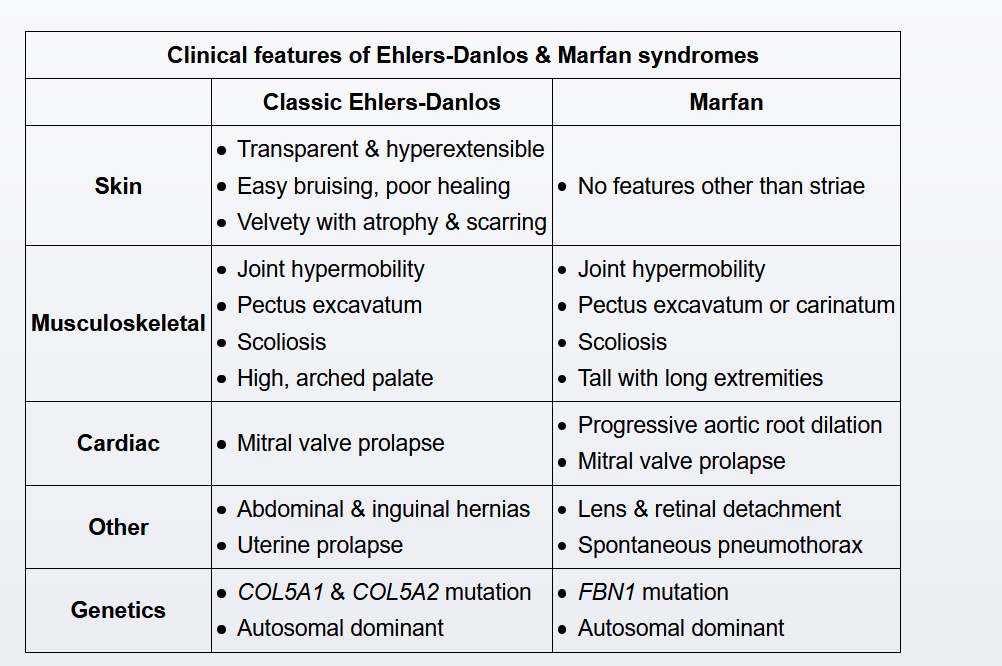
This patient most likely has Ehlers-Danlos syndrome (EDS), a connective tissue disorder characterized by joint hypermobility, recurrent joint dislocations, hyperextensible skin with easy bruisability, and delayed healing with atrophic scars. Patients may have associated skeletal abnormalities, including thoracolumbar scoliosis, pectus excavatum, and pes planus. Other features include hernias, cervical insufficiency, and uterine prolapse. Mitral valve prolapse with myxomatous degeneration of the valvular apparatus is a complication of EDS and can lead to rupture of the chordae tendineae and acute mitral valve regurgitation (MR).
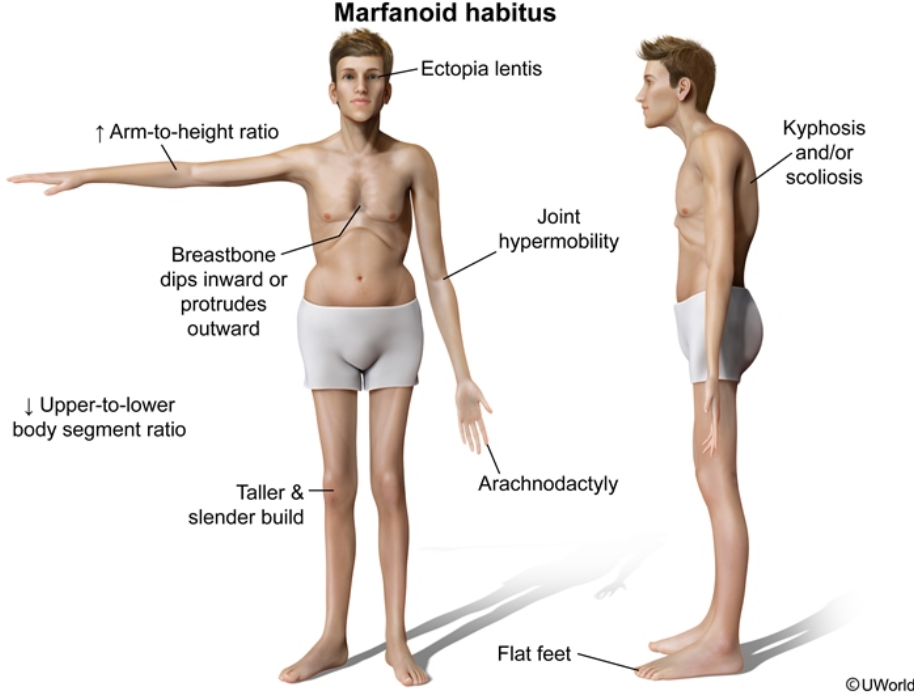
Marfan syndrome shares many features with EDS. Both diseases can cause scoliosis as well as myxomatous mitral valve degeneration and chordae tendineae rupture, leading to acute MR. However, skin findings are much less prominent in Marfan syndrome; this patient's velvety skin with atrophic scarring is consistent with EDS.
MRI/MRA of the brain can identify berry aneurysms, which occur more commonly in Ehlers-Danlos syndrome, in contrast to aortic aneurysms in MFS. Joint hypermobility and skin hyperextensibility are characteristic of Ehlers-Danlos syndrome.
The main cause of morbidity and mortality in patients with MFS is aortic root disease, manifesting as aneurysmal dilation, aortic regurgitation, and/or dissection. Patients with suspected MFS require an echocardiogram prior to sports participation. If aortic root disease and/or a family history of aortic dissection or sudden death is present, patients are counseled to avoid strenuous physical activity, with intense/contact sports (eg, track, basketball, football) generally restricted.